Filgotinib can help to get Colitis under control and keep it under control. Having your Colitis under control is known as remission. It can also reduce the need for long-term steroid treatment. But filgotinib does not work for everyone.
Clinical trial results
The information below shows the results of clinical trials. These looked at how effective filgotinib is. To find this out, scientists compared people who took filgotinib with people who took a placebo. A placebo is a substance that looks the same as the treatment but does not have any medicine in it.
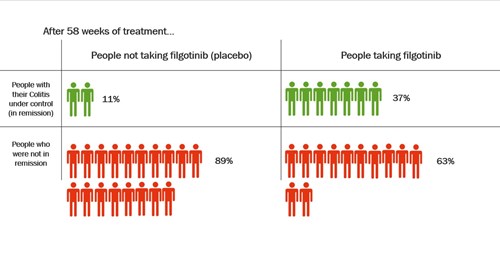
After around one year of treatment with filgotinib, an average of nearly 4 in every 10 people, or 37%, were in remission.
Of those who took a placebo, an average of around 1 in every 10 people, or 11%, were in remission.
This shows that more than three times as many people had their Colitis under control after taking filgotinib for one year, compared with people taking a placebo. But filgotinib did not work well for everyone with Colitis.
The table below shows data from clinical trials of filgotinib in adults with moderate to severely active Colitis.
Click to view at full size
Results from other research
One study looked at how well filgotinib worked long-term. In people who responded to filgotinib, 80% continued to be in remission after more than three and a half years.
Another study found that filgotnib may work better in people who have not tried biologics before.
Filgotinib has not been compared directly with other treatments for Colitis.
Find out more about how we talk about the effectiveness of medicines.